At TheHealthBoard, we're committed to delivering accurate, trustworthy information. Our expert-authored content is rigorously fact-checked and sourced from credible authorities. Discover how we uphold the highest standards in providing you with reliable knowledge.
What is Pulmonary Stenosis?
 Tricia Christensen
Tricia Christensen
Tricia Christensen
Tricia Christensen
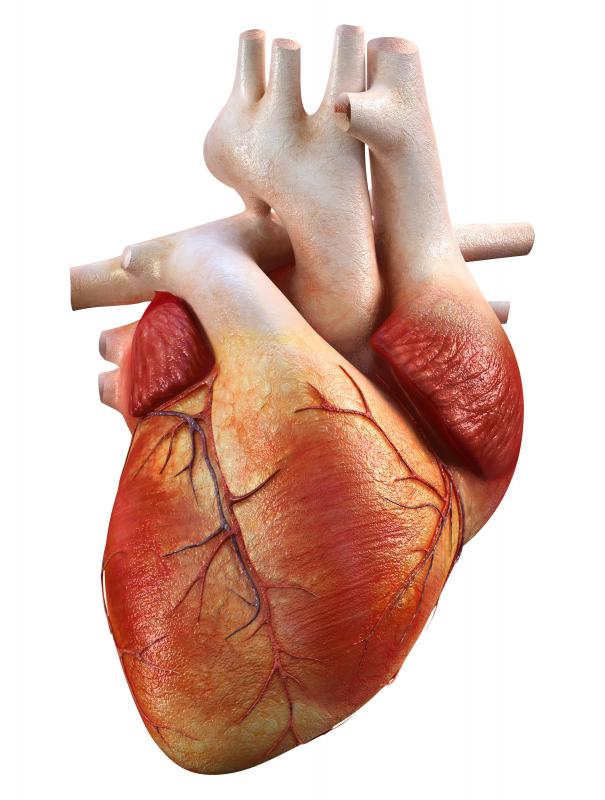
The pulmonary valve is attached to the right ventricle of the heart. It is the passageway through which blood flows to get to the lungs for oxygenation. Pulmonary stenosis, a congenital heart defect, is a narrowing of the leaflets of this valve, or of the valve itself. The leaflets open as the right ventricle contracts and pushes blood to the lungs, but when they are stenotic, the leaflets can stick or remain partially closed. Pulmonary stenosis is the most common of valve defects.
In many cases, pulmonary stenosis is mild and the narrowing does not significantly inhibit blood flow to the lungs. Peripheral pulmonary stenosis narrows the valve itself, but is generally mild. Such mild cases usually never require treatment, although physicians may hear a heart murmur when a stethoscope is applied to the chest of a newborn. The risk with more serious forms of pulmonary stenosis is back up of fluid into the heart and veins, and the need for the right ventricle to pump harder to move blood into the lungs. Over time, the extra work the heart is doing can result in heart failure.

The most common intervention for treating pulmonary stenosis is non-surgical. During a cardiac catheterization, a small balloon attached to the catheter is threaded through the heart to the pulmonary valve and then inflated to reduce narrowing. This treatment, balloon valvuloplasty, has a high degree of success. It also has the advantage of being an outpatient procedure when successful.

Sometimes balloon valvuloplasty is not enough. The procedure may be attempted to address the pulmonary stenosis, but may not be successful. If pulmonary stenosis still exists, several surgical options are available. The most common option is to excise the valve and replace it with either a pig valve, or a human valve from a cadaver. Unlike other transplants, rejection is not a factor in this surgery.

Children with this type of surgery generally do extremely well, but the valve does not grow with them, so at some point replacement of the valve is necessary. With most children, this may be done about ten years after the initial valve placement. Valve replacement, though it sounds serious, is considered a fairly routine procedure by most cardiothoracic surgeons.
Survival rates are excellent for valve replacements. Because of the artificial valve, cardiologists recommend antibiotics before dental procedures. Additionally, a child may be placed on long-term aspirin to prevent clots from forming in the new valve. The child will need to see a cardiologist yearly. This physician will assess the degree to which the new valve is working, and also determine when the valve might need replacement.
A child with pulmonary stenosis rarely needs immediate intervention right after birth. Pulmonary stenosis affects the heart over time, and the effect is varied by the degree of stenosis. Frequently, though, pulmonary stenosis is present with other defects, as in Tetralogy of Fallot, or hypoplastic right heart syndrome. In these cases, surgery may need to be performed shortly after birth to address these other defects.
Tricia Christensen
Tricia has a Literature degree from Sonoma State University and has been a frequent TheHealthBoard contributor for many years. She is especially passionate about reading and writing, although her other interests include medicine, art, film, history, politics, ethics, and religion. Tricia lives in Northern California and is currently working on her first novel.
Learn more...
Tricia Christensen
Tricia has a Literature degree from Sonoma State University and has been a frequent TheHealthBoard contributor for many years. She is especially passionate about reading and writing, although her other interests include medicine, art, film, history, politics, ethics, and religion. Tricia lives in Northern California and is currently working on her first novel.
Learn more...AS FEATURED ON:
AS FEATURED ON:

-
![Pulmonary stenosis is a narrowing of the leaflets of the pulmonary valve.]() By: adimasPulmonary stenosis is a narrowing of the leaflets of the pulmonary valve.
By: adimasPulmonary stenosis is a narrowing of the leaflets of the pulmonary valve. -
![Aspirin is sometimes prescribed in an effort to prevent blood clots.]() By: blueskies9Aspirin is sometimes prescribed in an effort to prevent blood clots.
By: blueskies9Aspirin is sometimes prescribed in an effort to prevent blood clots. -
![The circulation of blood from the heart to the lungs for oxygenation and back to the heart.]() By: silotoThe circulation of blood from the heart to the lungs for oxygenation and back to the heart.
By: silotoThe circulation of blood from the heart to the lungs for oxygenation and back to the heart.


Discussion Comments
To w.G. Writer:
my son's diagnosis is hypo-plastic right heart, tricuspid astrisea with a.S.D. (Atrial septal defect). When he was first born i was told his pulmonary artery was large enough so he would not need to have this first surgery. This "first surgery" was explained to me to be the b.T. Shunt. No one ever mentioned a banding until he was about 7 days old. By the way, jack was born over the memorial day holiday so most of the doctors were not available. During his first week of life jack's condition was very good. He was not even on o2. Then it seemed as soon as the doctors returned to work after the holiday jack's conditioned worsened, or in their opinion it did. However, his vitals, pao2, everything that was monitoring him the week prior was the same. The thoracic surgeon was sure he was going into congestive heart failure.
Please keep in mind, i am at their mercy and have no choice but to believe in these people caring for my son. The day of the pulmonary banding was awful. The surgery took a very long time and didn't go very well. Ever since that day jack's condition deteriorated. He started having episodes of clamping down when he was upset. His saturation was supposed to be in a range of 75 to 85. His would drop to 60, sometime even lower. Every breath he took he retracted. Before the banding this never occurred. When the surgeon explained this operation to me he said he would place the band on loosely so jack could grow into it. It was supposed to last 4 to 6 months. His lasted only 4 weeks and each day it was on he nearly died. I kept insisting that something was very wrong and finally they agreed to perform a heart cath because they believed a hole in his heart might be closing and this procedure would correct his problems. Well, the cath was done and again jack nearly died but it did nothing to relieve jack's problems.
We stayed in this hospital 3 months, jack's episodes continued on a daily basis. One morning, much to my surprise jack's doctor informed me we were being released. I was scared to death. Even on the day jack was released he again had another episode. We were sent home on o2, propranolol, digoxin and lasix along with a few reflux medications. Everyday we were home he would have these terrible episodes where he could not breath. His nail beds hands and feet would start turning blue. His legs would start modeling, finally he would become so exhausted his eyes would roll back and he would just pass out. I would hold the o2 over his nose and mouth and as he relaxed his o2 level would come back up and he would go to sleep. We went through this every day we were at home. Within 10 days we were back at the hospital. That night jack coded and he underwent an emergency surgery to remove the band. Removing the band did help some, but the scar tissue where the band had been still blocked enough blood flow so that he still had severe difficulty breathing and his pao2 was dangerously low.
We were so scared of the doctors and staff at this hospital i ask to be transferred to childrens hospital in arkansas where he had his glenn shunt. Now, jack is doing much better compared to his condition before. Karen
Dear Karen,
I truly feel for the difficult situation you are in, and for your whole family.
Obviously as writers we can only comment generally on definitions, and can't give medical advice. My suggestion to you is that if you feel the surgery was not appropriate, you have your son's records reviewed by a different physician, perhaps one not associated with the hospital that treated your son.
But recognize that there are many different approaches to treating congenital heart defects. Not all doctors or surgeons recommend the same approach, and sometimes, despite a surgeon's best efforts, things go wrong. That's tremendously difficult to accept as a parent, especially when a child does badly during a surgery.
With banding, usually the point is to create a degree of pulmonary stenosis so that bloodflow to the lungs will be restricted. In some heart conditions, this is necessary or pressure to the lungs can cause damage that can't be repaired, and makes heart lung transplant the only choice to fix a problem. But even under the best of circumstance, there are instances where things go wrong, despite qualified surgeons and the most advanced surgical techniques. Having a review of what was done might be helpful for you, because I know as parents we often blame ourselves for these choices (though really we didn't have much choice to begin with). Accept my best wishes to you and your family during this very difficult time.
What surgery should be performed to correct Pulmanary stenosis at birth?
Can the surgical procedure, Pulmonary artery banding, if done incorrectly, cause Pulmonary stenosis. In my baby's case, the band was placed too tightly around the artery. Because of the inadequate blood flow to His lungs He almost died. Several times, even after the band was removed the scar tissue caused by the band rendered him unable to breathe. Finally, his Pulmonary Artery collapsed and he coded, taking the Doctors and nurses over 15 minutes to even somewhat stabilize Him. He now has a bleed in the right frontal lobe of his brain and his future is uncertain.
I don't believe Jack, my son, ever needed this pulmonary artery banding. Should He have undergone a taussig shunt instead, which would have provided a temporary way for blood to get to the lungs.
Please give my your opinion.
Thank you, Karen Organ
Post your comments